In our last GKIS article, Is Your Child Screen Addicted? we discussed the definitions of screen addiction, who’s to blame, who is commonly afflicted, and what the brain studies say. Our next question is, OK then what? It turns out that inpatient treatment facilities for screen addiction are popping up all over Asia. We are starting to see the same here in the United States. When should you get help and what does help look like?
When to Get Help
GKIS supports parents to set family rules and promote healthy screen use before digital injury and addictive use occur. If you are concerned about your child’s relationship with their screens, the chart below is a great place to start. Read through each level of functioning and determine which best describes your loved ones.
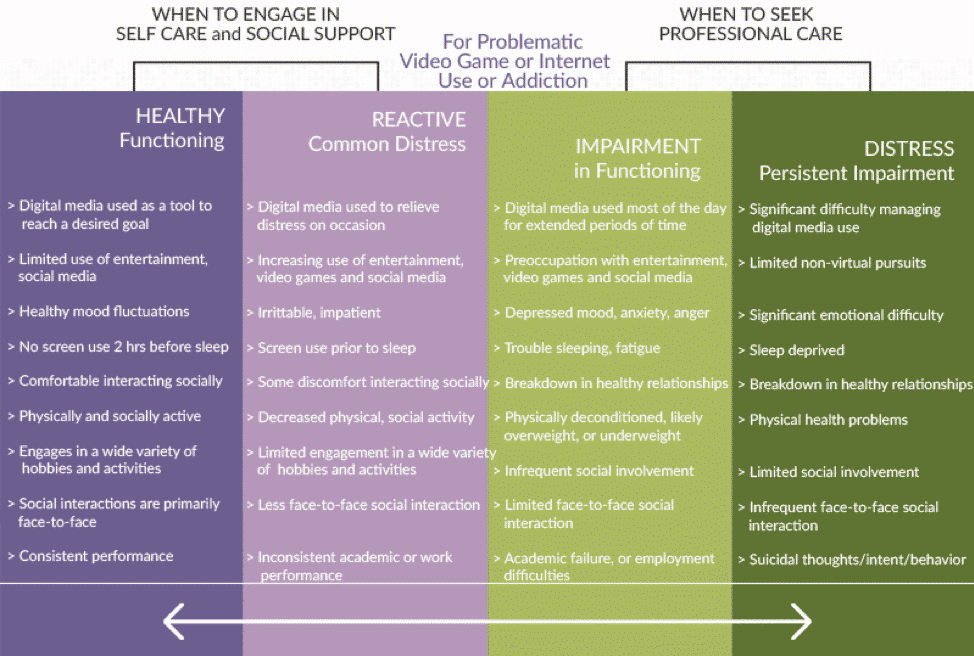
Fortunately, most kids fall under the reactive category for screen use. To avoid progression into Impairment or Distress, GKIS offers tools like our Screen Safety Essentials Course. If you think you’d like to get outside help as well, here are some facts that will help you navigate as you find the specific help you need.
Where can people with screen addiction go for treatment?
Outpatient Treatment
“Outpatient” simply means treatment from an office or clinic rather than admission to a hospital. Youth inpatient treatment programs are more expensive than outpatient and do not typically admit clients until they are at least 12 years old. If your child is young, and it’s early enough that the problem seems resolvable, outpatient services are the best place to start. Find an experienced professional like Dr. Bennett that will work with you and help family members implement follow-up care and make appropriate changes in the home.
Outpatient treatment starts with a comprehensive individual and family evaluation. They will then propose a treatment plan rich in cognitive behavioral coping skills (like those we offer in our Social Media Readiness Course). Usually, the practitioner will see you and your child once a week or twice a week in crisis situations. If your child needs more support, their mental health professional will refer you to extra resources or a partial outpatient or inpatient program. Partial outpatient typically refers to a program with multiple services available more than once a week.
Inpatient Treatment
Inpatient treatment usually involves an overnight stay away from home. Programs are typically offered in timeframes lasting 30, 45, or 90 days and include problem-focused, goal-directed therapies to address the symptoms of the individual’s problematic tech use. Clinicians guide clients through the process of “disconnecting and finding themselves.”
For a long-term stay, you may want to look into programs with accredited education so that your youngster can stay on track in school during treatment. Programs work to encourage a healthy balanced lifestyle while addressing underlying issues contributing to emotional factors (depression, anxiety, ADHD, ASD). Each client’s treatment plan should be individualized and created collectively by the client, their clinicians, and the family. All programs except aftercare should require their clients to be 100% tech-free while in treatment.
The following services have been shown to successfully treat behavioral addiction:
- Cognitive Behavioral Therapy (CBT)
- Individual and Group Psychotherapy
- Nutrition and Fitness
- Interpersonal Skills Groups
- Life Skills Psychoeducation
- Mindfulness-Based Stress Reduction (MPSR) & Meditation
- Guided Meditation Groups
- Yoga
- 12-Step Recovery Groups
- Relapse Prevention
- After Care Planning
- Family Workshops
During inpatient treatment, professionals will work to better understand the complex nature of the individual’s digital media abuse and how it is affecting their development, as well as address the underlying medical and mental health conditions. Patients spend time examining their close interpersonal relationships and how their thoughts, feelings, and behaviors are connected. By exploring patterns of thinking that lead to self-destructive actions and the beliefs that direct these thoughts, patients can modify their patterns of thinking to improve coping skills. Redirecting negative thinking is imperative for self-change, and, due to the immature neural networks in young people, they need more support to achieve lasting cognitive restructuring. Negative thinking patterns also exacerbate anxiety, depression, and compulsive behaviors.
It is important to shop around for quality and fit. Make sure that all treating professionals share an open line of communication with one another, the patient, and the family. As a team, they should help employ a balanced life plan for the client during and post-treatment. They will also go over the risks and benefits of use, potential relapse obstacles and triggers, and help the patient build familial and community connections which are imperative in maintaining a healthy sustainable lifestyle.
Who does the treatment?
Counselors
Counselors focus on overcoming substance abuse and maintaining sobriety. They tend to focus on the here and now and are typically not trained to work with mental health issues directly. Counseling activities include facilitating group therapy and support groups, family counseling for rebuilding and support, and individual counseling to manage symptoms, cravings, and triggers. Counselors work in outpatient and inpatient rehabilitative programs as well as transitional living environments like sober living homes.
Specific types of counselors:
- Substance abuse and behavioral disorder counselors provide treatment and support for those struggling with addiction. Education and licensing requirements vary by state. However, they typically have an associate degree and a substance abuse counselor certification. Some additionally seek a bachelor’s or master’s degree.
- School counselors typically have a bachelor’s degree, a teaching credential, and a two-year master’s degree. They specialize in front-line identification of student problems and individual and group counseling about broader issues, like academic and family issues.
Therapists
Therapists focus on mental and emotional health over time, of which substance abuse may be a part. Therefore, they treat mental health issues that co-occur with addiction, including mood and anxiety disorders. Therapists train with a variety of techniques. However, when working with addiction issues they primarily focus on cognitive behavioral therapy, contingency management, motivational enhancement, and individual and family behavioral therapy. Therapists typically work in private practices and outpatient and inpatient rehabilitative programs.
Specific types of therapists:
- Licensed marriage and family therapists (LMFT) and licensed professional clinical counselors (LPCC) have bachelor’s and master’s degrees. LPCC’s treat a broader scope of mental health issues, while LMFT’s focus on issues that stem from marriage and family relationships.
- Licensed clinical social workers (LCSW) are part of the mental health counseling branch of social work. They are required to get extra accreditation and training after receiving their master’s in social work (MSW) degree. MSW and LCSW therapies are designed to work with the client to discover what strong natural skills and talents they possess that can be used as a launching point to tackle the issues the client is facing. This process begins with an assessment phase that inventories the strengths and perceived challenges as well as the client’s environment. Then the LCSW works with the client to make and work toward realistic goals (immediate & long term) as well as work to improve the client’s relationship with others and themselves. Social workers can diagnose and provide therapy but cannot prescribe meds.
Licensed Clinical Psychologists
Psychologists typically have a Ph.D. (5-year degree) or PsyD (4-year degree) and are trained for testing and treatment. They have the training to deal with more serious mental illnesses than other treatment providers. Psychologists are often in supervisor and program development and management roles.
Psychiatrists
Psychiatrists are medical doctors that specialize in the diagnosis and treatment referrals for individuals with mental illness. They earn their medical degree and then attend five years of residency specialty training with clients with mental illness. They can prescribe medication and monitor/make dosage adjustments as needed.
Physicians
Physicians with a specialty in addiction medicine are medical practitioners that specialize in chemical and behavioral dependency.
Quick Tips for Parents and Kids in Recovery

Remember that they are doing something important and challenging! Kids making it through childhood and adults doing their best to parent…these are life’s hardest tasks. Blame is not useful, but courage, hope, and love are where it’s at.
“Rehab didn’t cure me of my disorder, but I do consider it to be the cornerstone of my recovery. It gave me a toolbox of coping mechanisms, others to relate to, a safe and open environment, and most importantly, the training to help me understand my specific plight and reframe my thinking. It was the starting point for the long and rigorous process of reclaiming my brain and thought patterns. It still took years after discharge for me to get truly healthy, but I do not believe without serious intervention I would not be where I am today. My disorder robbed me of my ability to connect with the world around me or manage stress without acting out. Today I can say I never imagined my brain to be released from those chains that tethered me to my addiction for so long…. and I owe much of it to the intense work I started in rehabilitation.”

I’m the mom psychologist who will help you GetKidsInternetSafe.
Onward to More Awesome Parenting,
Tracy S. Bennett, Ph.D.
Mom, Clinical Psychologist, CSUCI Adjunct Faculty
GetKidsInternetSafe.com
Photo Credits
Happy-kids United Way Lower Mainland CC 2.0
The pros and cons of giving an allowance Aaron Snider CC 2.0